Patients call at the clinic (the name of the IVF clinic is not disclosed for reasons of confidentiality) after leaving the site and throughout their treatment cycle to answer questions about their treatment protocol; more specifically, their requests are related to their preparation before the start of their treatment protocol, and to the medications to be taken and the tests to undergo during the treatment.
The IVF unit's administration is aware that the aforementioned increases operational costs and consumes part of their limited resources. They recognise that the adoption of new solutions and interventions may not only allow the clinic to follow the rapid changes taking place in the healthcare sector but also reduce costs while ensuring the provision of quality services that reply to patients' expectations.
Clinical staff and all those involved in the health care services are called upon to go beyond their comfort zone and offer a holistic experience of higher value required by individuals today.
Patient centricity requires questioning clinic's fundamental operating model and redesigning it with the end user at the core. In this case, research has been conducted in organisational level and throughout staff's interactions with the patients to reveal the non-profound causes of the problem.
The below principles have dictated the approach:
This methodology allowed us to deep dive into the entire patient journey and gain a higher level of patient and provider understanding.
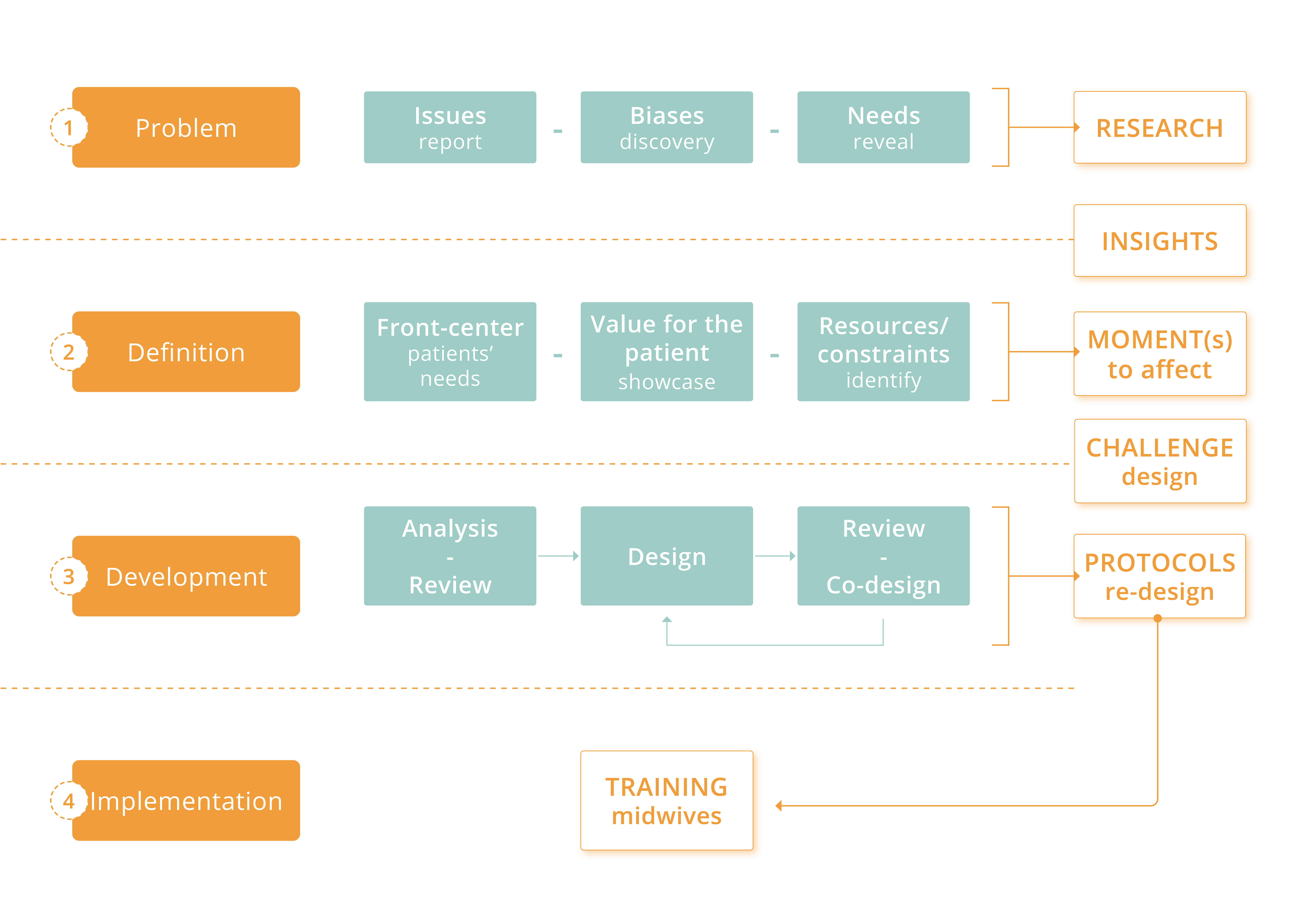
Aiming to bring a higher level of patient and provider understanding, primary and secondary research was conducted at clinic premises and outside of this. The methods incorporated observation of clinical personnel and patients’ interactions, interviews of staff in the different departments (midwives, head of secretaries, embryologist, biochemical laboratory staff), interviews with patients that had accomplished a treatment cycle, review of feedback forms, data analysis and documentation of the outcomes. Throughout an in-depth process, the causes of problems (initially reported by the clinic) were identified, biases affecting patients' behaviour were discovered, and structural & emotional needs of patients were revealed, as showcased on the patient journey map.
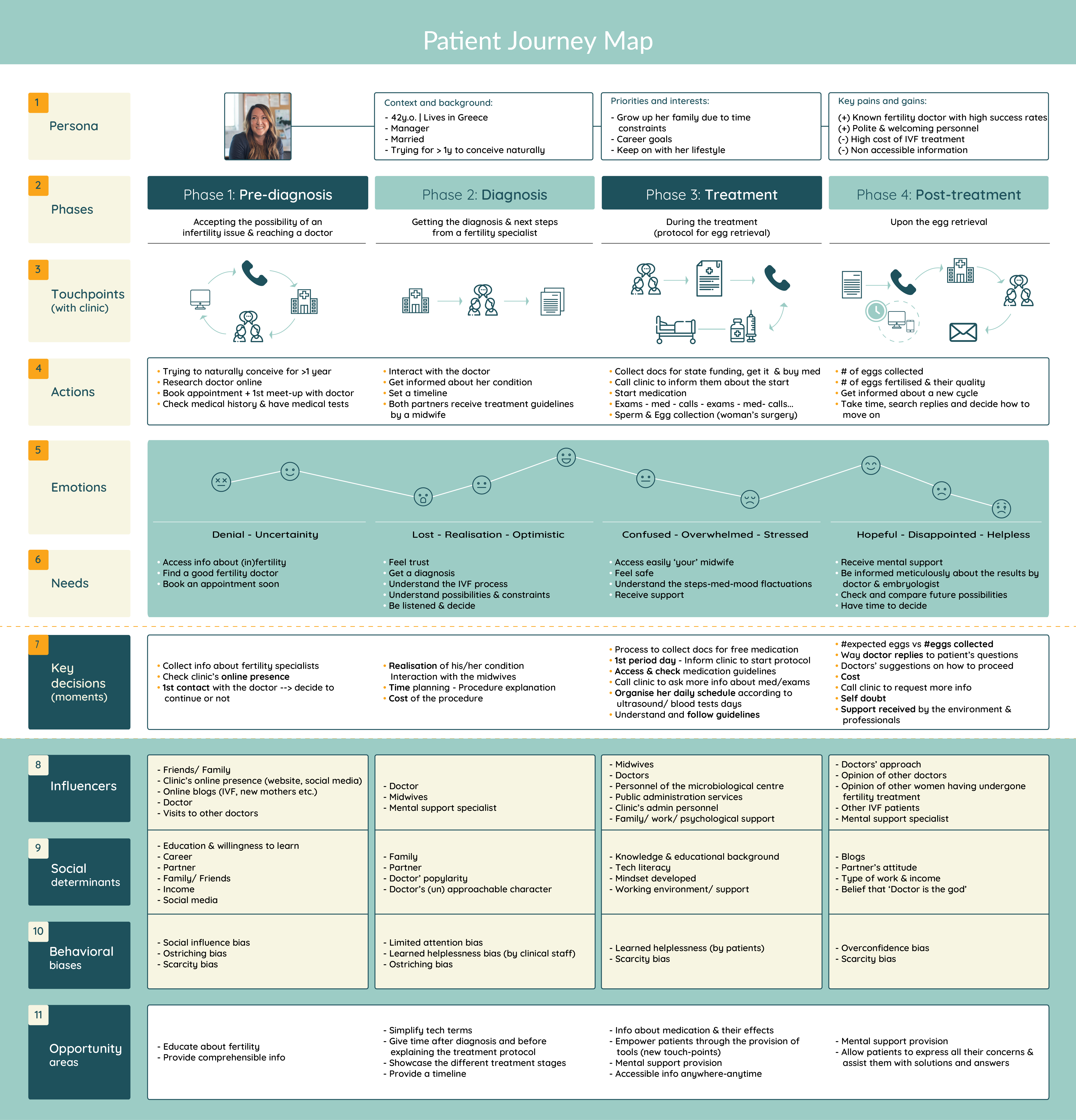
Note: Despite that the fertility journey of a patient starts long before the woman decides to visit an IVF clinic and finishes upon giving birth to her child, this patient journey map illustrates significant moments for the patient upon her decision to access a fertility doctor and till she completes the egg retrieval stage.
Upon collecting and analysing data, a set of insights were gathered for the patients, the staff and the interactions in between them.
The effective healthcare and delivery of treatment today incorporates medical expertise with social and behavioural understanding. Upon considering insights, constraints, opportunities and motivations, we identified the value across different moments, and defined the moments in the patient journey we can effectively influence to benefit both the patients and the clinic.

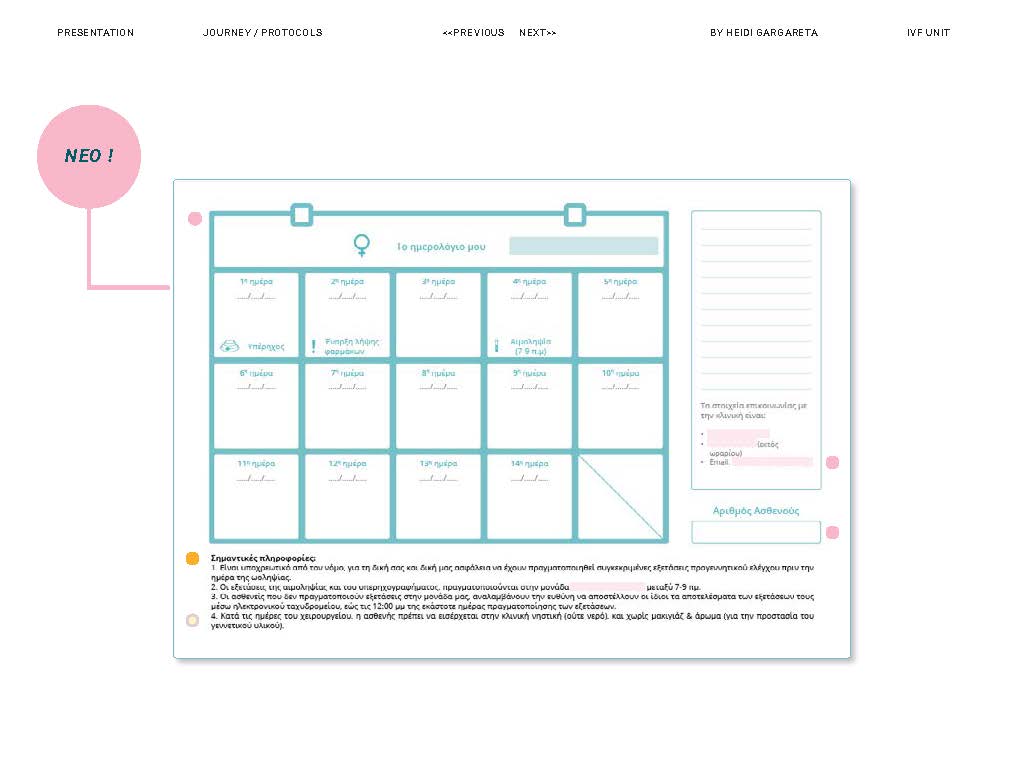
Upon establishing the new challenge, it became clear that the provision of tools to empower patients and turn them into active participants of their fertility journey is crucial towards a better experience for the patient, with significant and high-value results for the clinic.
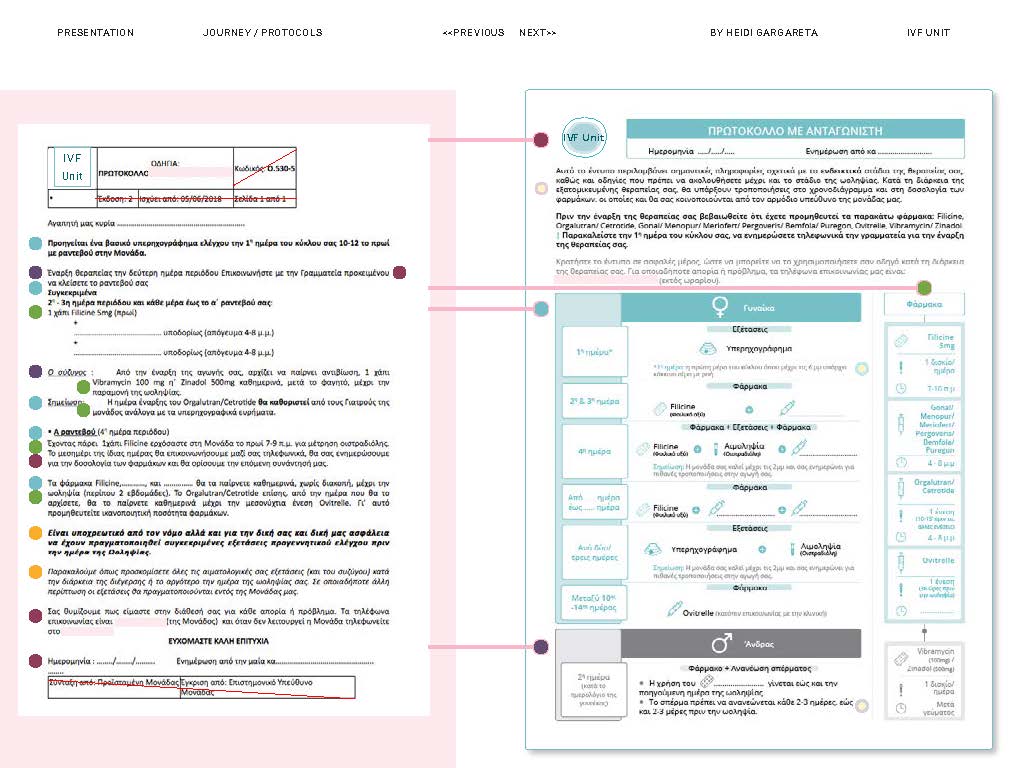
Towards this direction, various solutions were suggested, constraints were considered, and finally, redesign of the treatment protocols was realised to ensure patients' treatment adherence and better results for the clinic.
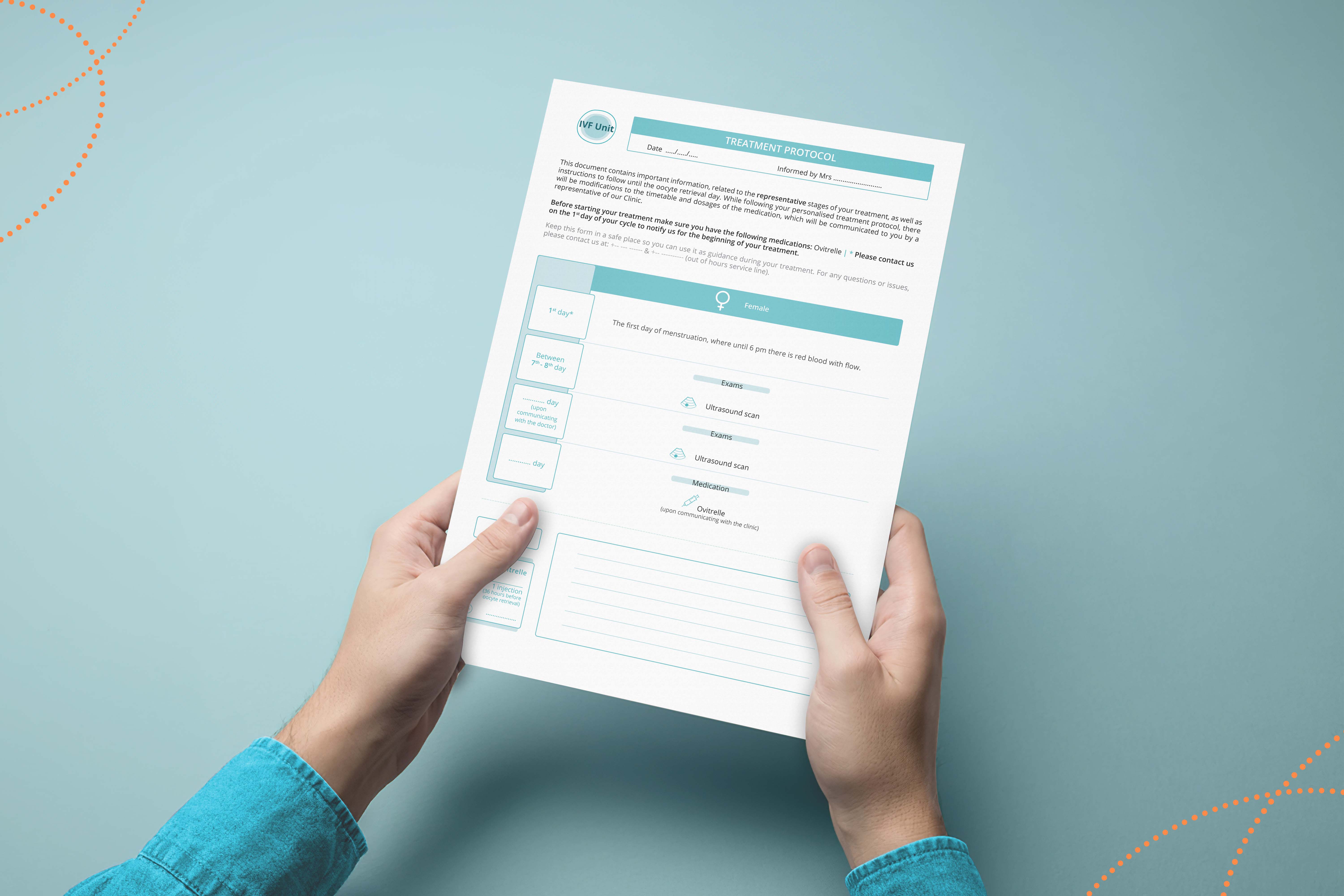
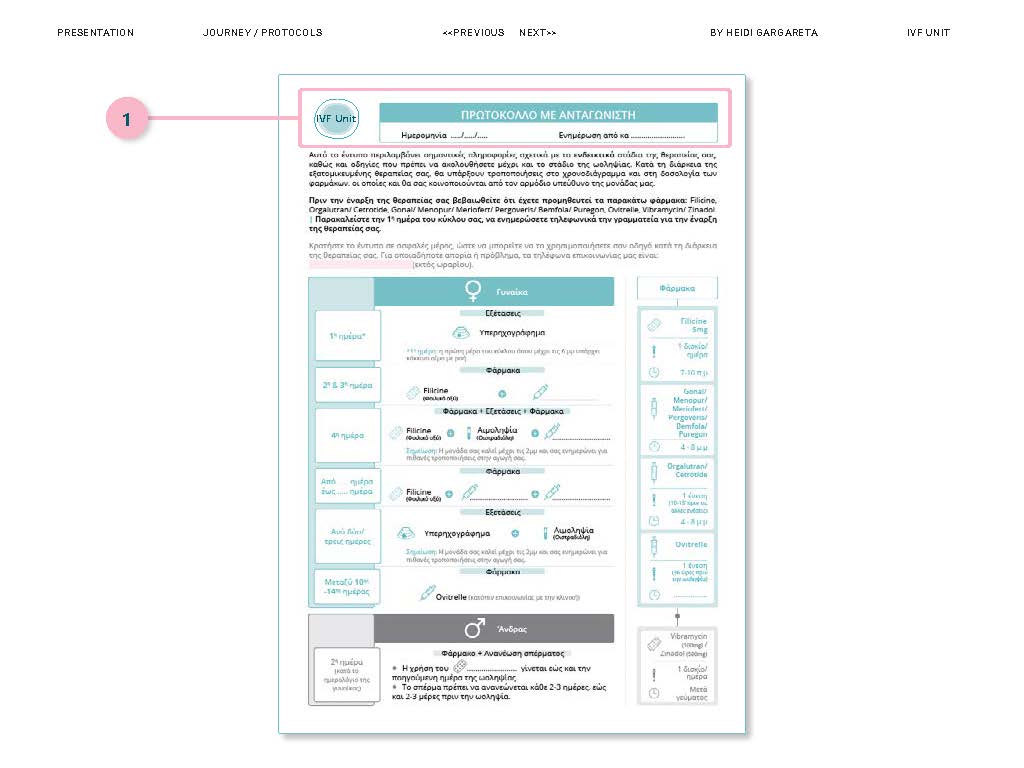
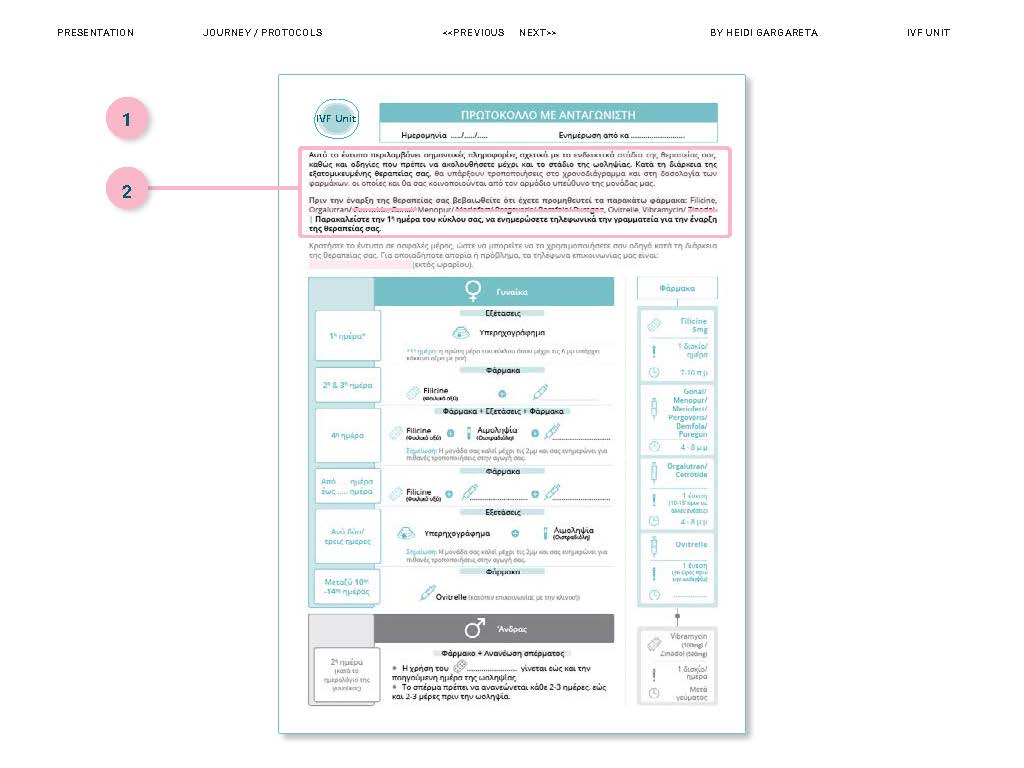
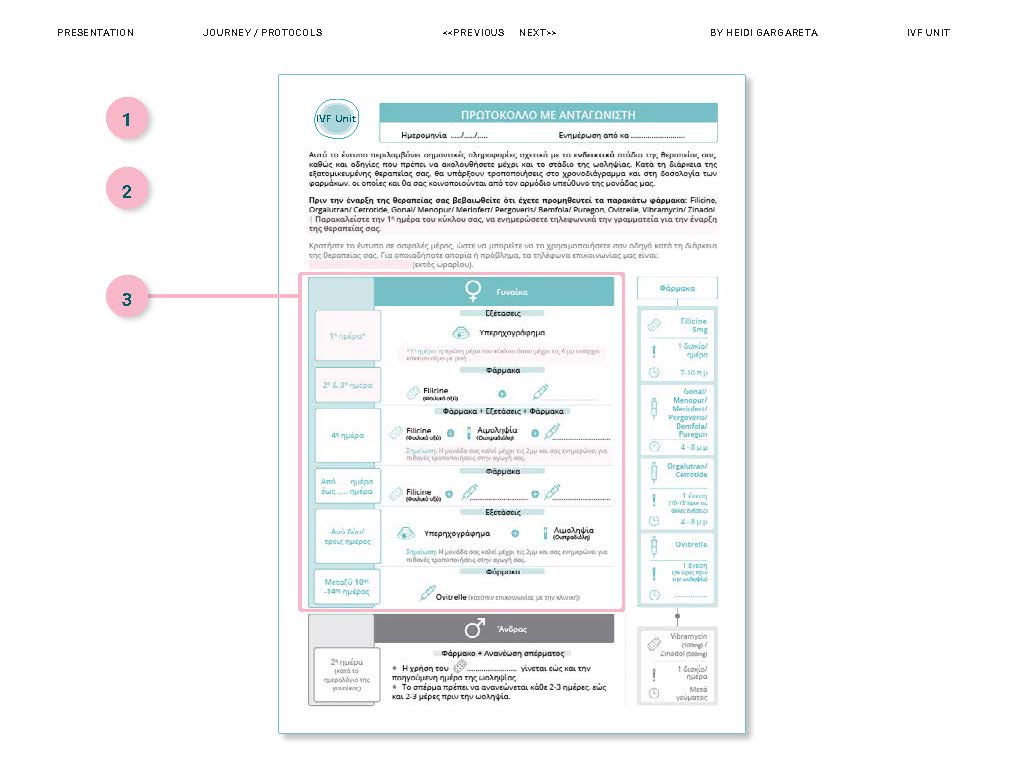
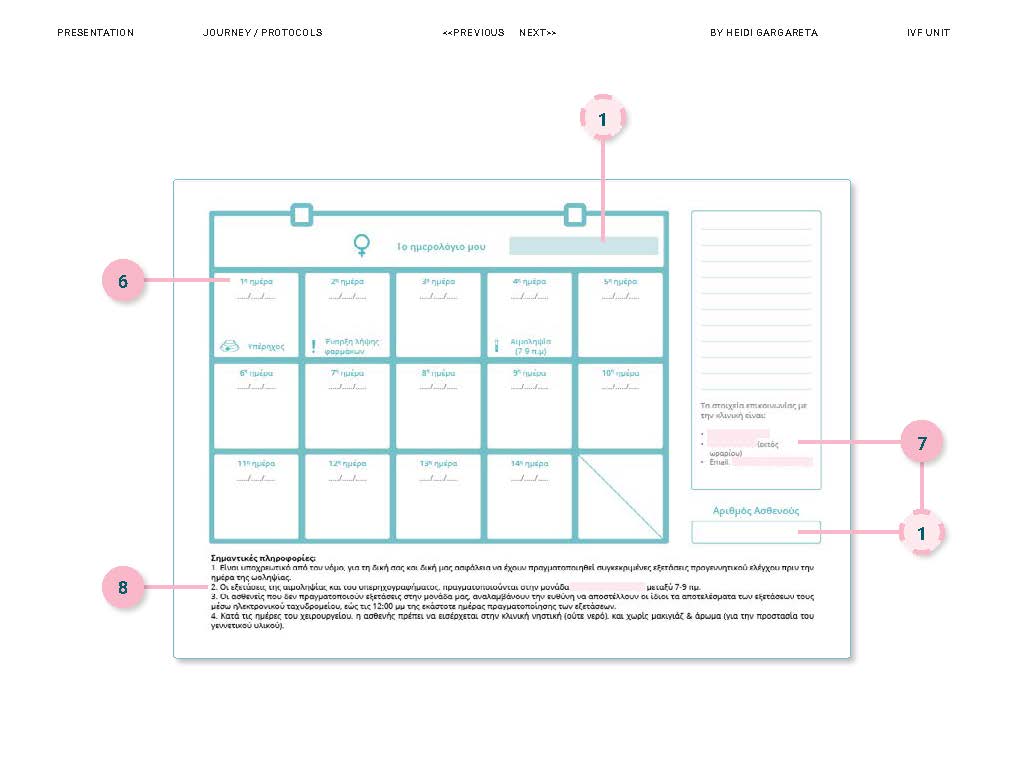
Treatment protocol documents need to incorporate specific, clear, and well-structured information, so that can serve their goal as a tool to guide patients during their fertility treatment cycle.
It seemed therefore essential to conduct in-depth research and analysis of the processes, in parallel with the review of the protocol documents. This took finally the form of an iterative co-design process between the service designer and the head of midwives; during this long-lasting process, there were also involved in different stages, the Head of secretaries, Accounting office representative, as well as an Embryologist whose role was to confirm the sequence of scientific processes and validate the information provided.
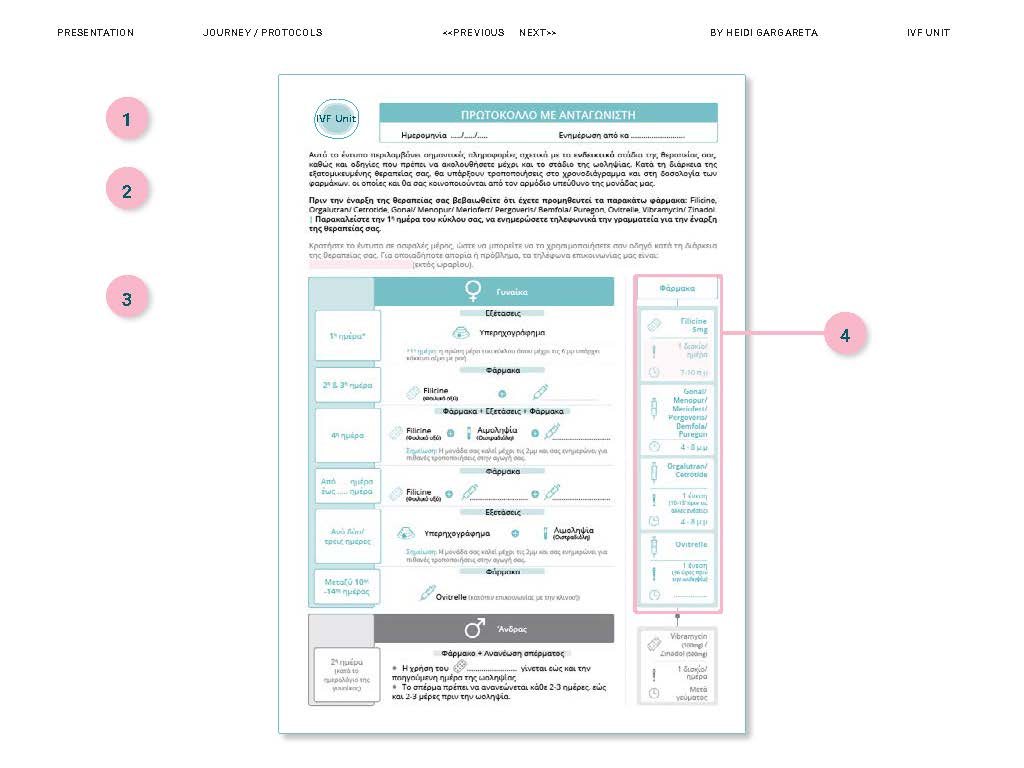
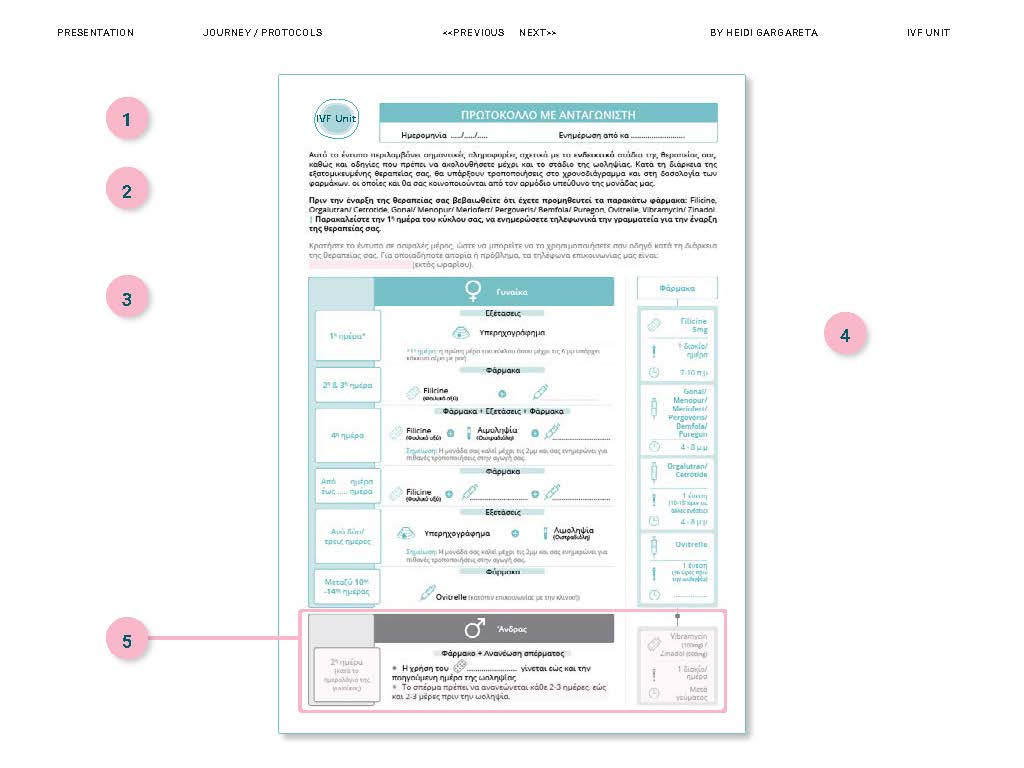
The focus was given on restructuring the existing information to make sense to the patient, and add the previously missing content in the document, essential for treatment adherence and for acknowledging the health care (eg. patient preparation before surgery) and administrative procedures taking place in the clinic.
Moreover, colour division of female & male partners' treatment guidelines was added, and icons were introduced to assist information navigation and recall by the patient.
The new treatment protocol documents (#16 in total) were designed with the patient at the core.
Goal Provide the tools to patients to empower them to become active participants of their own fertility journey, engaged in their own health care.
------------------------------------------------------------------------------------------------
Value
From presentation to training and future developments to allow automation in procedures and introduction of digital touchpoints to assist interaction between the patient and the clinic and better experience for both.
New treatment protocols were presented to the midwives (#9 in total) of the IVF clinic. They were given reasons for redesigning, as well as for the value of the new protocols for themselves and patients.
At the end of the presentation (delivered in greek language), the nurses were trained to understand the arrangement and content of the information, so that they could effectively communicate the instructions to the patients. Printed copies of all redesigned documents were given to them for further study after the end of the training session.

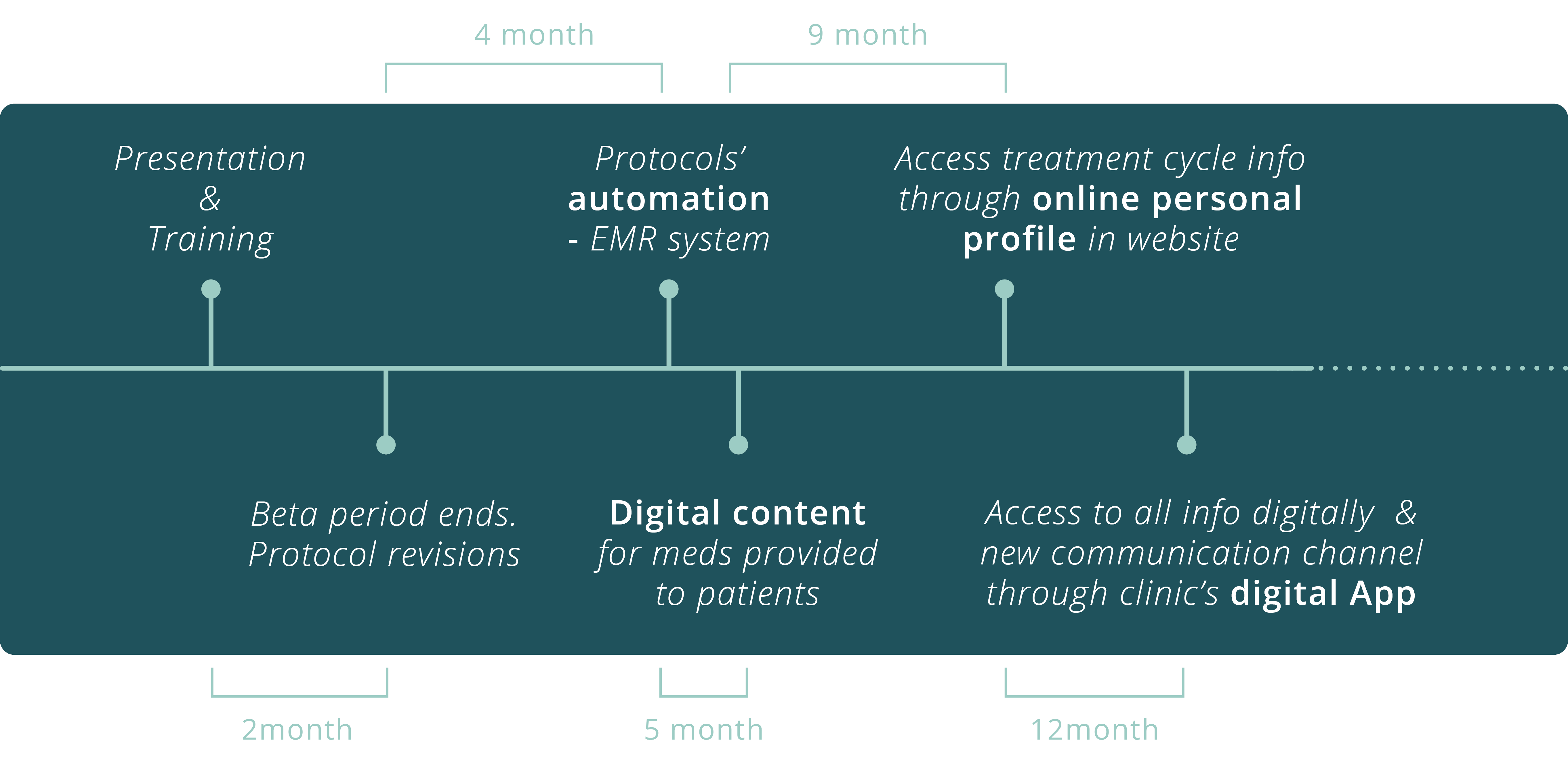
The timeline (according to clinic’s plans) indicates the steps for digitalising procedures internally -starting from the treatment protocols- to create better and more effective communication with the customers.
In fact, the new redesigned printed copies are being used as a first step to assist midwives' understanding towards the delivery of patient-centric healthcare services, before a partially automated procedure where personalised protocols will be automatically exported through the EMR system of the clinic. Later, patients will be able to access all this personal information along with other ones, online, through the clinic's website and App.
Performance indicators of this new touchpoint (hard copy) will dictate changes for future developments. Some of the below indicators may be used:
Lessons learned
- Working as a service designer in a traditional healthcare unit was challenging, as many staff members were unfamiliar with my role. Gaining the trust of key stakeholders, who acted as gatekeepers, was essential for collaboration and solution implementation.
- To achieve this, I clearly communicated research goals, shared evolving problems, and involved participants as informal co-partners, gathering their feedback at every stage. I avoided technical jargon and only introduced them to the design process once the challenge was clear and redesign decisions were made.
- Within this framework, protocol content was reviewed with department heads, and different layout versions were tested with clinical staff to ensure relevance and acceptance.
My role
UX researcher & Service Designer
My deliveries
16 protocols designs
3 additional docs design (incl. medical prescription, tests
prior IVF and obstetric booking sheet)
Content translation in English for all the documents
Presentation design & delivery
Training of midwives
Implementation steps & suggestions for further developments